Board Certification: American Board of Plastic Surgery
Fellowship-trained in Aesthetic Plastic Surgery
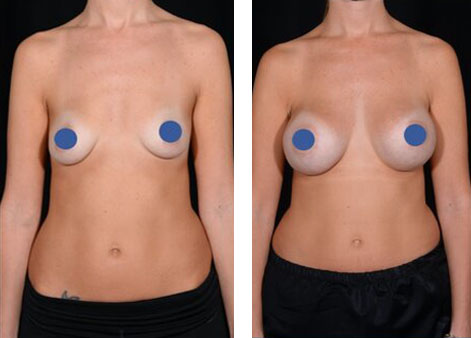
Aesthetic breast surgery includes making the breasts bigger (breast augmentation), smaller (breast reduction), or lifted (mastopexy).
There are several options to make the breast bigger. The most common way to make the breasts bigger is through the addition of an implant (breast augmentation). Current implants have a shell made of silicone and have a high safety profile. Within the silicone shell, breast implants are either filled with silicone or saline. There are pros and cons to both including implant feel, weight, detectability of rupture, and others. If a patient only wants a small augmentation and does not want an implant, they may be a candidate for autologous fat transfer to the breast. Like all procedures, there are risks and benefits that should be discussed prior to surgery. Overall, this can be a nice option for a small boost using your own tissue without the downside of a foreign body,
Breasts can also be made smaller and the nipple can be lifted. In general, a mastopexy (breast lift) is, by definition, a small reduction. Skin is removed to raise the nipple to a more youthful appearance. A varying amount of breast tissue is removed based on patient desires. For patients with back pain or other symptoms related to large breasts, certain insurances may pay for a breast reduction surgery.
Given the different options around aesthetic breast surgery, a consultation with a plastic surgeon can help a patient decide if an implant/fat grafting, lift/reduction, or both are needed to achieve their desired results.
A breast lift, also known as a mastopexy, is a popular option for individuals with excess skin and soft tissue of their breasts. This is especially true after pregnancy, menopause, and weight fluctuations. Many of these changes cannot be reversed by diet and exercise. As we age, the glandular breast tissue stretches and falls with gravity. The nipple-areola complex starts to point downward instead of forward. During a mastopexy surgery, the nipple is moved higher on the breast, the skin is tightened, and the breast tissue is lifted.
The short answer is no. There is no current substitute for removing unwanted skin and repositioning the breast tissue without the incisions typical of a mastopexy surgery. The amount of excess skin and the preoperative position of the nipple will dictate what type of incision is used and how much skin is ultimately removed. Anytime you cut the skin there will be a “scar.” With proper technique, the potential for well-healing fine scars is higher. Relative to other places on the body, breast skin tends to heal very well.
The incisions for a breast lift vary depending on the amount of tissue that needs to be removed. Going from least to most in terms of incision length (and final scar burden) is a periareolar incision, followed by a vertical incision or lollipop incision (periareolar plus a vertical lower midline incision), and lastly, a wise-pattern or anchor type incision which adds an additional incision in the inframammary crease (IMF).
A periareolar incision goes only around the nipple. This incision is good for several reasons. First, this incision hides very well at the junction between the pigmented tissue of the areola and the breast skin. Second, this incision can be used to make the areola smaller. Unfortunately, it is only possible to obtain a small lift from this incision only.
A lollipop breast lift is a periareolar incision plus a vertical lower midline incision. This is also referred to as a vertical breast lift or a vertical mastopexy. The periareolar incision generally hides well. The vertical incision is the most obvious incision on the breast but typically heals without issue and is very well tolerated. This incision helps to cone the breast and give it a more youthful, round shape.
A vertical breast lift or a vertical mastopexy is another way to describe a lollipop breast lift. The incision is a periareolar incision (around the nipple) and a midline vertical incision that typically heals without issue and is very well tolerated. This incision helps to cone the breast and give it a youthful shape.
A wise pattern mastopexy, also known as an anchor incision breast lift, combines the vertical breast lift (periareolar incision with midline vertical incision) and adds an incision in the inframammary fold (IMF). The IMF incision helps to remove excess skin and shorten the difference between the nipple and the fold. While this incision is the longest, it is also the most powerful in terms of skin removal and shape. In my opinion, the IMF incision is the least consequential of the three incisions as it hides very well in the fold underneath the breast. That being said, once a vertical incision is needed, the addition of an IMF incision should not dissuade a patient from this procedure or from a specific surgeon.
First, it is important to know if you truly want your nipples smaller or if you would like a reduction of the areola (pigmented tissue around the nipple). There are ways to make the actual nipple smaller including wedge excision and base reduction. More commonly, women complain of large areolas. Some women have large areolas at baseline. The areolas can get larger during life events like pregnancy/breastfeeding, puberty/breast growth, and weight gain. It is unlikely that the size of the areolas will reduce a significant amount after they have stretched. That being said, the areola size can be reduced with a periareolar incision. This is an incision hidden in the junction between the pigmented skin and the normal skin. The nipples can also be lifted several centimeters using this periareolar incision if needed.
A breast lift and a mastopexy are two ways to describe lifting the nipple to a more youthful appearance and reshaping the breast without a significant reduction in volume. Of course, the act of removing skin will reduce the breast volume and some additional breast tissue is usually removed to assist with creating a more youthful shape. That being said, a mastopexy or breast lift aims to keep the volume and reshape that volume. In a breast reduction, the nipple is lifted, the breast is reshaped, and breast tissue is removed from strategic areas to make the breasts smaller. These operations can be thought of on a spectrum. While insurance companies tend to consider a mastopexy a cosmetic procedure, breast reduction surgery is sometimes covered by insurance if certain criteria are met.
Breasts lifts are not typically covered by insurance. Breast lifts are considered a cosmetic procedure. If a significant volume of tissue is removed, this operation would be considered a breast reduction and may be covered by your insurance. Each insurance carrier has different criteria that need to be met in order to qualify.
Liposuction of the breasts is not an effective strategy for volume reduction. Breast tissue is fibrous and does not separate well with liposuction. There are some areas that can sometimes benefit from liposuction including mild fullness in the armpit and excess fat of the lateral breast/chest. Other than that, the breasts require excision procedures for areola reduction, nipple lift, tissue reshaping, and volume reduction.
Potentially. This is a decision that is discussed in your preoperative visit with your surgeon. Drains are small rubber tubes that help avoid excess fluid from accumulating in your body. While drains are a small inconvenience for a few days, drains help the recovery process. Some surgeons do not use drains. In my practice, I tend to avoid drains in breast lifts, mastopexies, and breast reduction surgeries unless there is a special circumstance.
A mommy makeover tends to be used to describe a tummy tuck performed in conjunction with aesthetic breast surgery. The aesthetic breast surgery could be a breast reduction, a breast lift (mastopexy), a breast augmentation (breast implants), or an augmentation/mastopexy (lift plus implants). A tummy tuck with a breast procedure is safe to do as long as your surgeon can do both cases in an expeditious manner.
Yes, you can have a mastopexy or breast lift before having children. That being said, I counsel my patient’s extensively and encourage them to wait until they are done have children to improve the final result. Even the best results can be compromised with weight loss, weight gain, or additional pregnancies. In contrast, many patients choose to undergo breast reductions prior to having children to improve back pain, posture, shoulder notching, and their overall quality of life.
All surgeons have slightly different protocols so each patient should follow their surgeon’s protocols. In general, breast lift patients should be treated similar to other major surgeries with the avoidance of strenuous activity and exercise for the first 4-6 weeks after surgery. Patients should walk frequently to attempt to avoid blood clots. Patients can power walk or get on a stationary bike as early as 2-3 weeks after surgery. The biggest issue that we hope to avoid by limiting certain activities is wound breakdown.
This is difficult to answer without a thorough conversation with a plastic surgeon. I tend to ask my patients if they have the volume that they want when wearing a non-padded bra. If the answer is yes, then they likely do not need an implant and instead they need a breast lift to raise the nipple and reshape the breast. That being said, if the patient wants upper pole fullness, then they may need a breast implant or the addition of fat grafting to the upper pole of the breast. A mastopexy alone will raise the nipple and improve the shape of the breasts but will not give upper pole fullness. A consultation with a plastic surgeon is recommended to determine the proper surgery to address your concerns and your expectations.
A breast reduction, also known as a reduction mammoplasty, is a popular option for individuals with excess skin and soft tissue of their breasts. This is especially true after pregnancy, menopause, and weight fluctuations. Many of these changes cannot be reversed by diet and exercise. As we age, the glandular breast tissue stretches and falls with gravity. The nipple-areola complex starts to point downward instead of forward. During a breast reduction surgery, the nipple is moved higher on the breast, the skin is tightened, and the breast volume is reduced. While some patients just want smaller breasts, others undergo breast reduction for symptoms of enlarged breasts (macromastia).
Symptomatic macromastia is a constellation of symptoms relating to the excess volume and weight of the breasts. Patients often complain of back pain, neck pain, shoulder pain, bra strap grooving or pigment changes, and breast pain. Patients can have poor posture from the weight and position of the breasts on their chest wall. Also, the patients can have rashes or skin problems on the undersurface of their breasts due to skin-on-skin contact (intertrigo). Reducing the volume and weight of the breasts and repositioning the breasts higher on the chest may help to improve some of these symptoms. No plastic surgeon can guarantee specific symptom relief after breast reduction surgery.
The short answer is no. There is no current substitute for removing unwanted skin and repositioning the breast tissue without the incisions typical of a breast reduction surgery. The amount of excess skin and the preoperative position of the nipple will dictate what type of incision is used and how much skin is ultimately removed. Anytime you cut the skin there will be a “scar.” The potential for well-healing fine scars is higher with proper technique. Breast skin tends to heal very well relative to other places on the body.
The incisions for a breast reduction vary depending on the amount of tissue that needs to be removed. There are two general types of breast reduction incisions. A vertical breast reduction, or lollipop breast reduction, is an incision around the areola and a vertical incision from the areola to the inframammary fold (IMF). A wise pattern, or anchor pattern, breast reduction is a vertical breast reduction pattern and an additional incision in the IMF.
A vertical breast is also referred to as a lollipop incision breast reduction. The incision is a periareolar incision (around the nipple) and a midline vertical incision that typically heals without issue and is very well tolerated. This incision helps to cone the breast and give it a youthful shape.
A wise pattern breast reduction combines the vertical breast lift (periareolar incision with midline vertical incision) and adds an incision in the inframammary fold (IMF). The IMF incision helps to remove excess skin and shorten the difference between the nipple and the fold. While this incision is the longest, it is also the most powerful in terms of skin removal and control of shape. In my opinion, the IMF incision is the least consequential of the three incisions as it hides very well in the fold underneath the breast. That being said, once a vertical incision is needed, the addition of an IMF incision should not dissuade a patient from this procedure or from a specific surgeon.
Yes. Some women have large areolas at baseline. The areolas can get larger during life events like pregnancy, puberty, and weight gain. It is unlikely that the size of the areolas will reduce a significant amount after they have stretched. That being said, the areola size can be reduced at the time of a breast reduction. There are different sizes plastic surgeons consider “normal.” Generally, this number is between 38 mm and 42 mm for the areola diameter but can be smaller or larger depending on the size of the breast. It is important to discuss the ideal areola size with your surgeon prior to undergoing a breast reduction surgery.
A breast lift and a mastopexy are two ways to describe lifting the nipple to a more youthful appearance and reshaping the breast without a significant reduction in volume. Of course, the act of removing skin will reduce the breast volume and some additional breast tissue is usually removed to assist with creating a more youthful shape. That being said, a mastopexy or breast lift aims to keep volume and reshape that volume. In a breast reduction, the nipple is lifted, the breast is reshaped, and breast tissue is removed from strategic areas to make the breasts smaller. These operations can be thought of on a spectrum. While insurance companies tend to consider a mastopexy a cosmetic procedure, breast reduction surgery is sometimes covered by insurance if certain criteria are met.
Sometimes. Your insurance company may cover breast reductions. Each insurance carrier has different criteria that need to be met in order to qualify. Your insurance carrier’s website will have more information on specific requirements.
Yes, you can have a breast reduction before having children. Many patients choose to undergo breast reductions prior to having children to improve back pain, posture, shoulder notching, and their overall quality of life.
Potentially. It is important to understand that up to 40% of patients will not be able to successfully breastfeed at baseline. During a breast reduction surgery, the nipple remains attached to some percentage of glandular tissue so it is possible to breastfeed successfully after breast reduction surgery. That being said, there is no way to guarantee this as a surgeon.
A breast surgery, depending on the complexity, takes around 1.5-3 hours. Additional operative time may be needed if another procedure is performed at the same visit. The total operative time may be longer when accounting for anesthesia time at the beginning and the end of the procedure.
A breast surgery is not a particularly painful operation but you may have some discomfort for several days. You will likely be swollen for the first several days after surgery. You will likely have a dressing on the incisions and a surgical bra to help keep weight off of the healing incisions. You will want to avoid any pushing, pulling, or other strenuous activity for the first few weeks. I advise my patients to avoid lifting anything heavier than 10 pounds (a gallon of milk) for the first several weeks after surgery.
All surgeons have slightly different protocols so each patient should follow their surgeon’s protocols. In general, breast lift patients should be treated similar to other major surgeries with the avoidance of strenuous activity and exercise for the first 4-6 weeks after surgery. Patients should walk frequently to attempt to avoid blood clots. Patients can power walk or get on a stationary bike as early as 2-3 weeks after surgery. The biggest issue that we hope to avoid by limiting certain activities is wound breakdown.